INTRODUCTION
The constriction of the horizontal part of the duodenum by the root of the mesentery or Wilkie’s syndrome (1-2), also known as vascular compression of the duodenum (3), produces a partial or total obstruction of the third portion of the duodenum, and it is manifested by abdominal pain, vomiting, loss of weight, and sometimes abdominal distension. It is an uncommon entity, which can compromise the patient’s life. For being infrequent it is not included in the initial diagnostic possibilities, which delays the diagnosis and appropriate treatment.
In this paper, we present a case in a 16-year-old male teenager, with a review the world literature, and we emphasize the clinical and imaging characteristics that allow to make its diagnosis. In our country, we found 6 publications (3-8) on this topic, which together collect a total of 7 cases.
CLINICAL CASE
The patient (CJ, 135866), a sixteen year old boy, with a history of 2 laparotomies, at 4 years of age for polytrauma with liver injury and at 10 years of age for adherent syndrome plus appendectomy, presented with abdominal pain, bilious vomiting on 20 occasions and radiological findings of partial intestinal obstruction Figure 1.

Figure 1. The X-ray of the standing abdomen shows dilatation of the stomach and few gas in the intestine distal to the point of obstruction, a characteristic image of a high partial intestinal obstruction.
On examination the patient appeared ill. His weight and height were 51 kg and 1.74 mt. He refers to the loss of 4 Kg in a month. A diagnosis of obstruction of the gastrointestinal tract by adhesions was made and in the laparotomy, multiple adhesions were found in the jejuno and ileon that obstructed the intestinal transit. Adhesions lysis was performed. Patient in the postoperative refers abdominal pain. A CT scan with contrast was performed demonstrating progression of the contrast until the rectal ampulla, treatment was established for a functional intestinal obstruction, paralytic ileus, without improvement; reason why intestinal transit was performed that showed a partial intestinal obstruction between the third and fourth portion of the duodenum Figure 2a and 2b.

Figure 2. a: shows cutoff of barium over spine, what indicates the narrowing of the horizontal part of the duodenum and few contrast and gas in the intestine distal to the point of obstruction.

Figure 2. b: shows gastroduodenal distension with the descending portion of the duodenum well distended and cutoff of barium to right of spine with delay in the emptying of the contrast and fight sign of the stomach.
The patient was underwent a laparotomy on 01-09-2012, and the intraoperative findings were: extensive adhesions between loops of small bowel that obstructed intestinal transit and a conglomerate of loops of small bowel on the horizontal portion of the duodenum without appreciating dilatation of the inframesocolic duodenum. We perform lysis of adhesions, and an intestinal plication using the Noble Operation technique. In the night of 01/13/2012 and early in the morning of 01/14/2012, the patient presented abundant vomiting of bilious color. The radiography of the abdomen performed shows dilatation of small bowel loops with air-fluid levels in the epigastrium and mesogastrium Figure 3.

Figure 3. The radiography of the abdomen shows dilatation of small bowel loops with air-fluid levels in the epigastrium and mesogastrium.
A Salem catheter was placed into the stomach and 1300 cc of bilious content was obtained. The patient was evaluated by the gastroenterology service that indicated treatment with prokinetic drugs; the bilious residue persisted in a volume of 2000 cc daily, despite treatment with prokinetic drugs. As of 01/20/2012, the patient had fever, attributed to the colonization of the catheter through which he received parenteral nutritional support. On 01/21/2012, an enteroscopy was performed, finding a narrowing between the third and fourth portion of the duodenum that did not allow the endoscope to pass through. Figure 4.
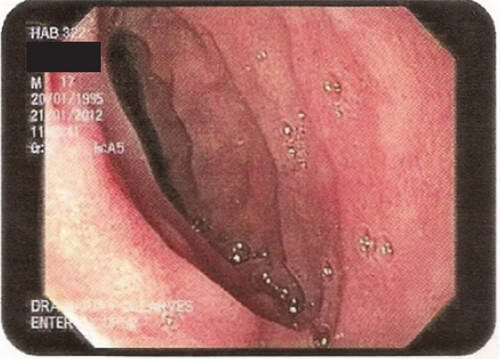
Figure 4. Enteroscopy shows the narrowing of the horizontal part of the duodenum that did not allow the endoscope to pass through.
We reviewed computerized axial tomography (TAC) and observed a decreased in angle and distance aortic mesenteric, with compression of the third portion of the duodenum. Figure 5.
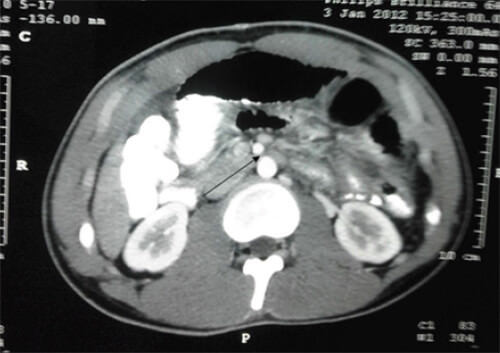
Figure 5. An axial cut of computerized tomography (TAC) shows a decrease in aortic mesenteric distance, with compression of the horizontal portion of the duodenum.
With the diagnosis of vascular compression of the horizontal part of the duodenum, we performed a laterolateral antecolic duodenojejunostomy, of the first jejunal loop to the descending part of the duodenum. Patient on the ninth postoperative day of the last surgical intervention, afebrile and tolerated oral feeding, we decided to discharge.
DISCUSSION
The constriction of the horizontal part of the duodenum by the root of the mesentery or Wilkie’s syndrome (1-2), also known as vascular compression of the duodenum (3), produces a partial or total obstruction of the third portion of the duodenum, and it is manifested by abdominal pain, vomiting, loss of weight, and sometimes abdominal distension. It is an uncommon entity, which can compromise the patient’s life. For being infrequent it is not included in the initial diagnostic possibilities, which delays the diagnosis and appropriate treatment. Most of the literature indicates that Rokitansky between 1842 and 1861 was the first to describe this entity (9-10), but Bermanski (11) who performed a very complete review of the Historical Background, indicates that: 1.- the first description of the superior mesenteric artery syndrome was made by Boernerus in 1752; 2.- Rokitansky in 1842, described the acute dilatation of the stomach resulting from compression of the duodenum by the root of the mesentery. 3.- Stavely in 1910 was the first to practice a successful duodenojejunostomy in a patient with gastro-mesenteric ileus. But it is not until 1921 when Professor Wilkie (1) publishes with the chronic duodenal ileus title, a series of 4 patients with three deaths and post-morten analysis and makes a very complete description of this entity and among the conclusions it should be noted that: 1.- Chronic duodenal ileus from compression of the third part of the duodenum by the root of the mesentery is a clinical and pathological entity and 2.- that the drainage of the dilated duodenum by duodenojejunostomy is the most certain method of treatment, and the only one suited for well-developed and late cases. Subsequently In 1927, Professor Wilkie published a series of 75 patients (2) and in 64 duodenojejunostomy was performed with three deaths and with satisfactory results in 80.70% of cases. After these two publications, the compression of the horizontal portion of the duodenum by the root of the mesentery is known worldwide as Wilkie’s Syndrome.
The incidence of vascular compression of the duodenum is low, between 0.0024% and 0.53% (12). It occurs most frequently in female sex and in children and young adults. In the etiopathogenesis of this disease are distinguished predisposing and precipitating factors (13). The predisposing factors are: an abnormally acute aortomesenteric vascular angle with a short superior mesenteric artery, abnormally high fixation of the duodenojejunal angle by the Treitz ligament, exaggerated lumbar lordosis, unusually low origin of the superior mesenteric artery, supine position, variations in the location of the horizontal portion of the duodenum (14); and the precipitating factor is the marked decrease in body weight with loss of mesenteric and retroperitoneal fat, which reduce the angle and the distance aortic mesenteric from its normal values from 28º to 65º and from 10 to 34 mm, at an angle less than 22º and a distance less than 10 or 8 mm (15), which produces the compression of the horizontal portion of the duodenum. In normal persons, the average of the aortic mesenteric angle ranges from 60º to 45º with an average of 56º, while the measurements of the persons with vascular compression of the duodenum vary between 10º to 22º, with an average of 14.67º (14).
Vascular compression of the duodenum is clinically manifested by post-pandial fullness, abdominal pain, vomiting, weight loss and sometimes abdominal distention (12,16-18). The clinical manifestation depends on the degree of duodenal obstruction. When the degree of obstruction is slight, the symptoms are postpandrial fullness, nausea, and sometimes vomiting that may not contain bile, and when the degree of obstruction is greater appear: the abdominal pain located in the epigastrium and vomiting with biliary contents, that can be incoercible. Abdominal distention occurs in intense degrees of obstruction and is a manifestation clinical of a severe gastric dilatation.
For being infrequent, initially the attending physician does not think about it, which delays diagnosis and treatment. The diagnosis is made by radiological studies, endoscopy and computed axial tomography and requires a careful evaluation and high index of suspicion. The radiography of the abdomen standing can show dilatation of the stomach and duodenum with few gas in the distal intestine to the point of obstruction (19), Fig. Nº 1, or a massive dilatation of the stomach and proximal duodenum, with absence of gas distal to the point of obstruction in the duodenum (20). The radiological study of the gastrointestinal tract shows: 1.- the narrowing of the horizontal part of the duodenum over the spine or to the right of the spine (21), Fig Nº 2a y 2b, 2.- few contrast and gas in the intestine distal to the point of obstruction, 3.- gastroduodenal dilatation with delay in the emptying of the contrast and fight sign of the stomach, Fig. Nº. 2a-b. Normally, the second portion of the duodenum empties the barium so quickly, that it is difficult to obtain a radiograh that shows the descending portion of the duodenum well distended. In patients with vascular compression of the duodenum, this portion of the duodenum remains distended (19) Fig Nº 2b. The endoscopy of the upper digestive tract shows the narrowing of the horizontal part of the duodenum Fig. 4. The axial and reconstructed images of the computed tomography allow: 1.- to demonstrate gastroduodenal dilatation with a narrowing of the third portion of the duodenum between the superior mesenteric artery and the aorta, 2.- to determine the value of the angle and the distance aortic mesenteric and 3.- to rule out other causes of intestinal obstruction (15,22). There are discrepancies in the publications on the normal values of aortic mesenteric angle (15,22-23), reporting as normal, values between 28º and 65º; and it is consider abnormal when it is less than 25º (15,22-23). The aortic mesenteric distance in normal people varies between 10 and 34 mm and it is considered abnormal when it is less than 8 to 10 mm (15,23).
The treatment of vascular compression of the duodenum depends on the grade of the obstruction and the patient’s tolerance. A group of patients respond to medical treatment while others require surgical treatment (24). Medical treatment consists of gastric decompression and nutritional support. Successful nutritional support using a naso jejunal feeding tube inserted endoscopically that exceeded the obstruction has been reported (25). Medical treatment is successful in 78.1% of cases (26). The surgical treatment is indicated, when the medical treatment is not successful (26-27) or when there is clinical manifestations of intestinal obstruction. There are several modalities of surgical treatment: 1.- duodenojejunostomy (1,2,27); 2.- section of the suspensory muscle of the duodenum with descent of the horizontal portion of the duodenum (28); and 3.- duodenal derotation (29). 4.- gastrojejunostomy is not recommended because the contents of the duodenum (biIe and pancreatic juice) before of the obstruction, needs to regurgitate to the stomach, to be drained into the jejuno (30,31).
In the surgical intervention, sometimes, it is not appreciated dilatation of the duodenum nor the area of obstruction, as it happened in our case, and is useful to show the level of obstruction, the insufflation of 150 to 200 cc of air through a nasogastric tube (30,31).
The surgical treatment most frequently practiced is that proposed by Professor Bloodgood (32) and popularized by Professor Wilkie (1,2), the laterolateral duodenojejunostomy.
REFERENCIAS
- Wilkie DPD: Chronic duodenal ileus. Br J Surg 1921;9:204-214. https://doi.org/10.1002/bjs.1800093405
- Wilkie DPD: Chronic duodenal ileus. Am J Med Sci 1927; 173:643-649.
- Acosta-M B, Guachalla G, Martínez C, Felce S, Ledezma G. Compresión vascular del duodeno. GEN 1991; 45(1):61-64.
- Trejo-Padilla E. Cirugía del Tubo Digestivo en el Niño. Tribuna Médica de Venezuela 1976;45(5):41-48.
- Sánchez Ismayel A, Cohén D, D’Amelio C, Daly K, Sánchez R, Salas J. Síndrome de Arteria Mesenterica Superior: Causa Inusual De Obstruccion Duodenal. Vitae 2007;32. Available from: http://vitae.ucv.ve/index_pdf.php?module=articulo_pdf&n=1136.
- Bandres D, Ortiz A, Dib Jr. J. Superior mesenteric artery syndrome. Gastrointest Endosc 2008; 68(1):152–153. Available from: https://doi.org/10.1016/j.gie.2007.09.033.
- Vassallo M, Marín J, Hernández Y, Chaparro ML, Malave H.Síndrome de la arteria mesentérica superior. Reporte de un caso y revisión de la literatura. Rev Fac Med 2010;33(2):159-163. Available from: http://190.169.30.98/ojs/index.php/rev_fmed/article/download/4909/4720.
- Mota M, Abusaid S, Muñoz C. Síndrome de Wilkie: a propósito de un caso. CIMEL 2014; 19(2):91-95. Available from: https://www.cimel.felsocem.net/index.php/CIMEL/article/download/491/297.
- Welsch T, Büchler MW, Kienle P (2007). “Recalling superior mesenteric artery syndrome”. Dig Surg. 24 (3): 149–56. doi:10.1159/000102097.
- Lorentziadis ML. Wilke’s syndrome. A rare cause of duodenal obstruction. Annals of Gastroenterology (2011) 24, 59-61. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3959462/pdf/AnnGastroenterol-24-59.pdf
- Bermanski Paul, Golden Richard L, Ricca Richard J. Superior Mesenteric Artery Syndrome Complicated by Pancreatitis. A Case Presentation and Historical Background. Vascular Surgery 1995;29(3):217-23. http://journals.sagepub.com/doi/pdf/10.1177/153857449502900308.
- Townsend Jr. CM, Naoum JJ. Chapter 83 Vascular Compression of the Duodenum. In Fischer JE. Editors. Mastery of Surgery. 5th Edition Lippincott Williams & Wilkins 2007. p. 955-961.
- Ahmed AR, Taylor I. Superior mesenteric artery syndrome. Postgrad Med J. 1997;73(866):776-8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2431524/pdf/postmedj00156-0010.pdf. doi: 10.1136/pgmj.73.866.776
- Akin JT Jr, Skandalakis JE, Gray SW. The anatomic basis of vascular compression of the duodenum. Surg Clin North Am. 1974;54(6):1361-70. Available from: https://doi.org/10.1016/S0039-6109(16)40491-3
- Agrawal GA, Johnson PT, Fishman EK. Multidetector row CT of superior mesenteric artery syndrome. J Clin Gastroenterol 2007;41(1):62-65. Available from: https//doi.org/10.1097/MCG.0b013e31802dee64
- Anderson JR, Earnshaw PM, Fraser GM. Extrinsic Compression of the Third Part of the Duodenum. Clin Radiol 1982;33(1):75-81. Available from: https://doi.org/10.1016/S0009-9260(82)80358-9
- Chang J, Boules M, Rodriguez J, Walsh M, Rosenthal R, Kroh M. Laparoscopic duodenojejunostomy for superior mesenteric artery syndrome: intermediate follow-up results and a review of the literature. Surg Endosc. 2017;31(3):1180-1185. Available from: https://doi: 10.1007/s00464-016-5088-2
- Lee TH, Lee JS, Jo Y, Park KS, Cheon JH, Kim YS, Jang JY, Kang YW. Superior mesenteric artery syndrome: where do we stand today?. J Gastrointest Surg. 2012;16(12):2203-11. Available from: https://doi: 10.1007/s11605-012-2049-5
- Burrington JD, Wayne ER. Obstruction of the duodenum by the superior mesenteric artery — Does it exist in children? J Pediatr Surg. 1974;9(5):733-741. Available from: https://doi.org/10.1016/0022-3468(74)90112-2.
- Wayne ER, Burrington JD. Management of 97 Children With Duodenal Obstruction. Arch Surg. 1973;107(6):857–860. Available from: https://doi:10.1001/archsurg.1973.01350240027009.
- Burrington JD. Superior mesenteric artery syndrome in children. Am J Dis Child. 1976;130(12):1367-1370. DOI: 10.1001/archpedi.1976.02120130073015
- Gould R, Sandstrom CK, Strote J. Identification of superior mesenteric artery syndrome from vascular angle measurements. J Emerg Med. 2015;49(1):e35–e36. Available from: http://dx.doi.org/10.1016/j.jemermed.2014.12.087.
- Kothari TH, Machnicki S, Kurtz L.Superior mesenteric artery syndrome.Can J Gastroenterol. 2011 Nov;25(11):599-600. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3222767/. http://downloads.hindawi.com/journals/cjgh/2011/617201.pdf. doi: 10.1155/2011/617201
- Osegueda de Rodríguez EJ, Hernández-Villegas AC, Serralde-Zúñiga AE, Reyes-Ramírez ALDC. The two sides of superior mesenteric artery syndrome treatment: conservative or surgical management? Nutr Hosp. 2017 Jul 28;34(4):997-1000. Available from: http://scielo.isciii.es/pdf/nh/v34n4/33_nota.pdf doi: 10.20960/nh.1006.
- Chan DK, Mak KS, Cheah YL. Successful nutritional therapy for superior mesenteric artery syndrome.Singapore Med J. 2012 Nov;53(11):e233-6. Available from: https://sma.org.sg/UploadedImg/files/SMJ/5311/5311cr4.pdf
- Lee TH, Lee JS, Jo Y, Park KS, Cheon JH, Kim YS, Jang JY, Kang YW. Superior mesenteric artery syndrome: where do we stand today?J Gastrointest Surg. 2012;16(12):2203-11. doi: 10.1007/s11605-012-2049-5.
- Mathenge N, Osiro S, Rodriguez II, Salib C, Tubbs RS, Loukas M. Superior mesenteric artery syndrome and its associated gastrointestinal implications.Clin Anat. 2014 Nov;27(8): 1244-52. doi: 10.1002/ca.22249.
- Strong EK. Mechanics of Arteriomesenteric Duodenal Obstruction and Direct Surgical Attack Upon Etiology. Ann Surg.1958;148(5):725-730. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1450911/
- Pillay Y. Superior Mesenteric Artery Syndrome: A Case Report of Two Surgical Options, Duodenal Derotation and Duodenojejunostomy. Case Rep Vasc Med. 2016;2016:8301025. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5215251/pdf/CRIVAM2016-8301025.pdf doi: 10.1155/2016/8301025.
- Jones SA, Carter R, Smith LL, Joergenson EJ. Arteriomesenteric duodenal compression. The American Journal of Surgery Volume 100, Issue 2, August 1960, Pages 262-277. https://doi.org/10.1016/0002-9610(60)90300-7
- Colina Cedeño OL, Trejo Scorza E, Brito Arreaza EJ. El Síndrome de Wilkie en Imágenes. Rev Cent Med. 2019;58(147):12-16.
- Bloodgood JC. Acute Dilatation of the Stomach-Gastro-mesenteric Ileus. Ann Surg.1907;46(5):736-62. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1414443/ doi: 10.1097/00000658-190711000-00011
